
🌸

🌸
What Is a Virus? - Dr. Lanka - VIRUS. - What is Coronavirus?
Virus Refuted. - Viruses - 1. - Viruses - 2. - Viruses - 3
Understanding Covid19. - The Virus Theory - Simple - Educational
🌸
"UNDERSTANDING Covid19"
https://ancientmistery.weebly.com/understanding-covid19.html
🌸
What is CORONAVIRUS?
🌸
What Is a Virus? - Dr. Lanka - VIRUS. - What is Coronavirus?
Virus Refuted. - Viruses - 1. - Viruses - 2. - Viruses - 3
Understanding Covid19. - The Virus Theory - Simple - Educational
🌸
"UNDERSTANDING Covid19"
https://ancientmistery.weebly.com/understanding-covid19.html
🌸
What is CORONAVIRUS?
🌸
🌸
Watch the VIDEO below ...
under a Microscope
your cells create the Corona Cell ...
Watch the VIDEO below ...
under a Microscope
your cells create the Corona Cell ...
🌸
An electronic Microscope is showing you
how a natural anti cancer killer cell,
when attacking a tumor,
LOOKS EXACTLY LIKE A
COVID -19 VIRUS CELL
this is filmed in real time.
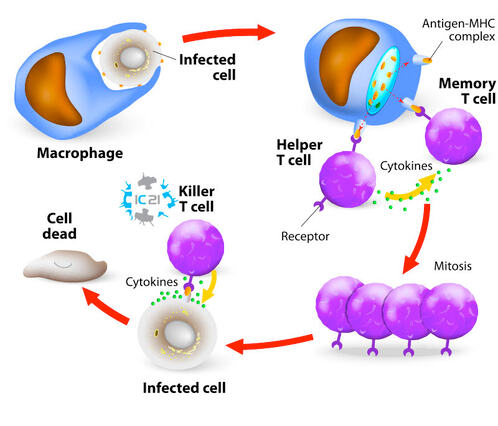
This is a video of a cellular immunity enhancement product
showing how our immune system works ...
around the 25 second mark of the video … and 53 second ...
you see round killer cells attack a tumor,
then you will see it magically turn into a “ coronavirus”
( which is not a VIRUS )
as the tumor brakes apart causing a corona around the offending tumor cell.
Once the cell is taken apart by the smaller immune cells,
the look of the offensive material has a
corona ...
🌸
THEY look very much like the CELLS,
that the Government & Medical System
want to kill the so called
"CORONAVIRUS"
🌸
An electronic Microscope is showing you
how a natural anti cancer killer cell,
when attacking a tumor,
LOOKS EXACTLY LIKE A
COVID -19 VIRUS CELL
this is filmed in real time.
This is a video of a cellular immunity enhancement product
showing how our immune system works ...
around the 25 second mark of the video … and 53 second ...
you see round killer cells attack a tumor,
then you will see it magically turn into a “ coronavirus”
( which is not a VIRUS )
as the tumor brakes apart causing a corona around the offending tumor cell.
Once the cell is taken apart by the smaller immune cells,
the look of the offensive material has a
corona ...
🌸
THEY look very much like the CELLS,
that the Government & Medical System
want to kill the so called
"CORONAVIRUS"
🌸
🌸
THIS IS BEING USED
TO LOCK YOU DOWN,
WEAR A MASK,
AND EVENTUALLY FORCE YOU
TO GET A VACCINE
🌸
BELOW IS A PICTURE OF THE CORONA
(FROM THE ABOVE VIDEO) WHICH IS THE TUMOR CELL’S
LAST GASP… BEFORE DYING.
🌸
See the picture below
at the 53 second of the Video ...
🌸
THIS IS BEING USED
TO LOCK YOU DOWN,
WEAR A MASK,
AND EVENTUALLY FORCE YOU
TO GET A VACCINE
🌸
BELOW IS A PICTURE OF THE CORONA
(FROM THE ABOVE VIDEO) WHICH IS THE TUMOR CELL’S
LAST GASP… BEFORE DYING.
🌸
See the picture below
at the 53 second of the Video ...
🌸

🌸
When you have tumors or toxic proteins in your system, these killer cells come out and digest the offending material … then dump them in your kidney or colon.
These proteins that are present are mostly from eating a toxic diet,
but these Killer Cells keep us all alive by literally eating the garbage and preventing further damage..
When you have such a toxic diet, your body creates excess mucus to prevent these acidifying proteins, from touching down on the soft tissues in your respiratory system,
by coating the soft cells with mucus …
Hence, you will have symptoms of what is called a
“Cold” or "Flu"
but is nothing more than the body trying to dump these toxins from your system.
These symptoms include a fever which, tries to burn the proteins from your blood.
🌸
In other words,
what the Government & Medical system is calling
a VIRUS is their own creation …
🌸
You create the disease with ...
Electronics, telephone, and WIFI pollution.
Lack of Sunshine - Vitamin D.
Lack of Exercise.
Stress.
🌸
Lack of Oxygen.
(from breathing indoor polluted air -
most items in our homes are made from toxic substances).
🌸
Toxic Food.
Fast Food.
Glyphosate Saturated Food.
Protein and starches eating in the same time producing very acidic body.
Pizza made with wheat and any wheat product.
🌸
Coca Cola, Pepsi Cola, Red Bull, etc.
Sugar.
Coffee.
Drugs.
Alcohol.
Etc.
🌸
Then these so called “coronavirus cells” which are really natural killer cells
are actually there to keep you alive.
🌸
If pharmaceutical companies ever create a vaccine
to destroy your Natural Killer Cells …
humanity will not last very long.
These proteins that are present are mostly from eating a toxic diet,
but these Killer Cells keep us all alive by literally eating the garbage and preventing further damage..
When you have such a toxic diet, your body creates excess mucus to prevent these acidifying proteins, from touching down on the soft tissues in your respiratory system,
by coating the soft cells with mucus …
Hence, you will have symptoms of what is called a
“Cold” or "Flu"
but is nothing more than the body trying to dump these toxins from your system.
These symptoms include a fever which, tries to burn the proteins from your blood.
🌸
In other words,
what the Government & Medical system is calling
a VIRUS is their own creation …
🌸
You create the disease with ...
Electronics, telephone, and WIFI pollution.
Lack of Sunshine - Vitamin D.
Lack of Exercise.
Stress.
🌸
Lack of Oxygen.
(from breathing indoor polluted air -
most items in our homes are made from toxic substances).
🌸
Toxic Food.
Fast Food.
Glyphosate Saturated Food.
Protein and starches eating in the same time producing very acidic body.
Pizza made with wheat and any wheat product.
🌸
Coca Cola, Pepsi Cola, Red Bull, etc.
Sugar.
Coffee.
Drugs.
Alcohol.
Etc.
🌸
Then these so called “coronavirus cells” which are really natural killer cells
are actually there to keep you alive.
🌸
If pharmaceutical companies ever create a vaccine
to destroy your Natural Killer Cells …
humanity will not last very long.
🌸
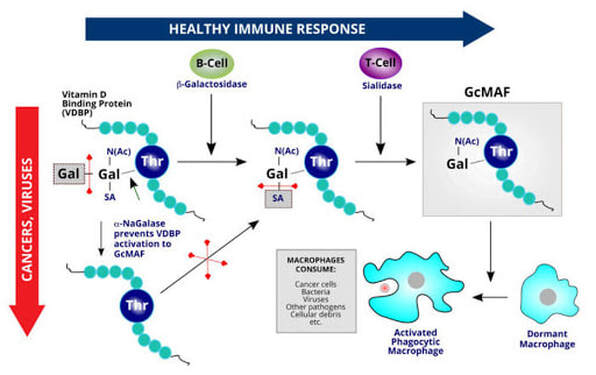
GcMAF is essential
to our immune system,
it is a protein that our bodies make
to destroy alien cells and toxins.
GcMAF is essential
to our immune system,
it is a protein that our bodies make
to destroy alien cells and toxins.
🌸
🌸
The Body Naturally Produce
GcMAF
🌸
GcMAF
🌸
https://healingoracle.ch/2019/08/28/11489/
GcMAF is essential to our immune system, it is a protein that our bodies make to destroy alien cells and toxins. All 5 billion healthy humans on the planet make their own GcMAF. The people with chronic illness do not produce enough, that is why they are sick.
A human makes 10,000 – 100,000 cancer cells a day, but your GcMAF,
which has six attacks on cancer, destroys them every day.
That is how it was designed. But modern life is changing this.
Globulin component Macrophage Activating Factor or GcMAF,
is also called vitamin D-binding protein-derived macrophage activating factor. It is an endogenous (occurring within the body) glycosylated vitamin D binding regulatory protein present within the immune system. This naturally occurring protein is found in all healthy individuals, but is depleted in people with an improperly functioning immune system.
Excitingly, GcMAF immunotherapy has been shown to improve immune system function – and quite possibly, prevent and even reverse cancer.
GcMAF is essential to our immune system, it is a protein that our bodies make to destroy alien cells and toxins. All 5 billion healthy humans on the planet make their own GcMAF. The people with chronic illness do not produce enough, that is why they are sick.
A human makes 10,000 – 100,000 cancer cells a day, but your GcMAF,
which has six attacks on cancer, destroys them every day.
That is how it was designed. But modern life is changing this.
Globulin component Macrophage Activating Factor or GcMAF,
is also called vitamin D-binding protein-derived macrophage activating factor. It is an endogenous (occurring within the body) glycosylated vitamin D binding regulatory protein present within the immune system. This naturally occurring protein is found in all healthy individuals, but is depleted in people with an improperly functioning immune system.
Excitingly, GcMAF immunotherapy has been shown to improve immune system function – and quite possibly, prevent and even reverse cancer.
🌸
🌸
🌸
https://steemit.com/health/@deepwaterscrypto/take-protein-gcmaf-and-get-rid-of-cancer
https://www.completewellnessreport.com/tragic-13-holistic-doctors-dead-in-4-months/
https://www.completewellnessreport.com/tragic-13-holistic-doctors-dead-in-4-months/
🌸

A study on infectivity of asymptomatic SARS-CoV-2 carriers – May 13,
2020https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7219423/
Respir Med. 2020 May 13 : 106026.
Ming Gao,a,∗,1 Lihui Yang,b,1 Xuefu Chen,c Yiyu Deng,d Shifang Yang,e Hanyi Xu,e Zixing Chen,e and Xinglin Gaoe
Abstract, Background
An ongoing outbreak of coronavirus disease 2019 (COVID-19) has spread around the world. It is debatable whether asymptomatic COVID-19 virus carriers are contagious. We report here a case of the asymptomatic patient and present clinical characteristics of 455 contacts, which aims to study the infectivity of asymptomatic carriers.
Material and Methods
455 contacts who were exposed to the asymptomatic COVID-19 virus carrier became the subjects of our research. They were divided into three groups: 35 patients, 196 family members and 224 hospital staffs. We extracted their epidemiological information, clinical records, auxiliary examination results and therapeutic schedules.
Results
The median contact time for patients was four days and that for family members was five days. Cardiovascular disease accounted for 25% among original diseases of patients. Apart from hospital staffs, both patients and family members were isolated medically. During the quarantine, seven patients plus one family member appeared new respiratory symptoms, where fever was the most common one. The blood counts in most contacts were within a normal range.
All CT images showed no sign of COVID-19 infection. No severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections was detected in 455 contacts by nucleic acid test.
Conclusion In summary,
all the 455 contacts were excluded from SARS-CoV-2 infection and we conclude that the infectivity of some asymptomatic SARS-CoV-2 carriers might be weak.
Keywords: SARS-CoV-2, Asymptomatic carrier, Contacts, Infectivity
2020https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7219423/
Respir Med. 2020 May 13 : 106026.
Ming Gao,a,∗,1 Lihui Yang,b,1 Xuefu Chen,c Yiyu Deng,d Shifang Yang,e Hanyi Xu,e Zixing Chen,e and Xinglin Gaoe
Abstract, Background
An ongoing outbreak of coronavirus disease 2019 (COVID-19) has spread around the world. It is debatable whether asymptomatic COVID-19 virus carriers are contagious. We report here a case of the asymptomatic patient and present clinical characteristics of 455 contacts, which aims to study the infectivity of asymptomatic carriers.
Material and Methods
455 contacts who were exposed to the asymptomatic COVID-19 virus carrier became the subjects of our research. They were divided into three groups: 35 patients, 196 family members and 224 hospital staffs. We extracted their epidemiological information, clinical records, auxiliary examination results and therapeutic schedules.
Results
The median contact time for patients was four days and that for family members was five days. Cardiovascular disease accounted for 25% among original diseases of patients. Apart from hospital staffs, both patients and family members were isolated medically. During the quarantine, seven patients plus one family member appeared new respiratory symptoms, where fever was the most common one. The blood counts in most contacts were within a normal range.
All CT images showed no sign of COVID-19 infection. No severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections was detected in 455 contacts by nucleic acid test.
Conclusion In summary,
all the 455 contacts were excluded from SARS-CoV-2 infection and we conclude that the infectivity of some asymptomatic SARS-CoV-2 carriers might be weak.
Keywords: SARS-CoV-2, Asymptomatic carrier, Contacts, Infectivity
Abbreviations:
COVID-19, Coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; CHD, congenital heart disease; EDOU, emergency department observation unit; ED, emergency department; CT, computed tomography; RT-PCR, Reverse Transcription-Polymerase Chain Reaction; GCDC, Guangzhou Center for Disease Control and Prevention; CDC, Chinese Center for Disease Control and Prevention; IQR, interquartile ranges; PPE, personal protective equipment
1. Introdution
The emergence of the coronavirus disease 2019 (COVID-19) since early December 2019, has spread to many countries recently and sparked world pandemic via mass gathering [[1], [2], [3]]. As of March 24, 2020, there have been 334981 confirmed cases and 14652 deaths globally [4].
It has been proved that the pathogen of COVID-19 is severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which has high homology with SARS-CoV [5]. Similar to SARS-CoV, the dominant SARS-CoV-2 transmission mode is human-to-human transmission [6].
Differently, the reproductive number (R0) (the expected number of secondary cases produced by a single infected person in a susceptible population) is estimated between two and three, which is higher than SARS [6,7]. Furthermore, the transmission of SARS occurs during the symptomatic period [8]. For COVID-19, numerous asymptomatic infections were found among close contacts of confirmed patients, like the report on “Diamond Princess” [9].
However, the epidemiological significance of asymptomatic infections is unclear until now. Recent studies indicated that transmission of COVID-19 could also occur from these individuals with no symptoms [10,11]. However, for now, whether asymptomatic SARS-CoV-2 carriers are contagious still remain controversial.
Here, we report a case of an asymptomatic SARS-CoV-2 carrier with nosocomial infection and describe the clinical characteristics of 455 contacts. Our purpose is to analyze the infectivity of asymptomatic carriers.; CASE PRESENTATION.
Case A was a 22-year-old female patient who had a medical history of congenital heart disease (CHD) presented to the emergency room of Guangdong Provincial People’s Hospital (Guangzhou, Guangdong province, China) on January 13, 2020. She complained of shortness of breath for 16 years, and the symptom worsened for one month. The accompanied symptom was chest distress, without cough, sputum production and fever. Apart from CHD, she had no other diseases and had no smoking habit. Her temperature was normal, and laboratory measurements showed no apparent abnormalities (Table 1 ). Echocardiography displayed atrial septal defect and severe pulmonary hypertension. The diagnosis was congenital heart disease, atrial septal defect and pulmonary hypertension.
Table 1
Laboratory measurements of Case A.
JAN, 13FEB, 12FEB, 19FEB, 27NORMAL RANGEBlood count, × 10⁹/L
White blood cell count7.707.787.417.923.50–9.50
Neutrophil count4.974.144.164.441.80–6.30
Lymphocyte count2.132.912.132.631.10–3.20
Serological variables
C-reactive protein, mg/L0.65.89NTNT<5.0
Procalcitonin, ng/ml Normal NormalN TNT<0.05Case A was mainly given to oxygen therapy, diuretic treatment, plus pharmacotherapy of pulmonary hypertension. On January 16, as Case A’s condition improved and vital signs became stable, she was transferred to emergency department observation unit (EDOU). Owing to the Spring Festival and COVID-19 outbreak, she had been hospitalized in EDOU along with her brother until February 11.
Before admission, she underwent a serious of examinations according to hospital-formulated guidance during epidemic period. Nevertheless, the patient’s nasopharyngeal swab tested positive for SARS-CoV-2 by real-time Reverse Transcription-Polymerase Chain Reaction (RT-PCR). She was immediately admitted to quarantine ward in infectious department.
Case A and her brother both denied visiting Wuhan (the epidemic area in China) and any contact with COVID-19 patients. They wore masks all the time except at meals and drinking. How she became infected was unknown.
Notably, in isolation, the patient had never fever, sore throat, myalgia or other symptoms associated with virus infection [12]. Shortness of breath and chest distress, without further aggravation than before, were thought to be caused by CHD. Laboratory measurements reflected that white blood cells, lymphocytes, C-reactive protein and procalcitonin were within a normal range (Table 1).
Upon admission, chest computed tomography (CT) scan showed non- COVID-19 imaging feature (Fig. 1 . a, c). In the time of hospitalization, the patient received antiviral and interferon therapy. 11 days after the treatment (February 22), chest CT scan indicated no significant differences in comparison with before (Fig. 1. b, d).
Chest CT images of Case A.
Figure a and c were taken on February 11, which showed non- COVID-19 imaging feature. Case A underwent a CT scan again on February 22. Figure b and d, the follow-up images, showed no significant differences than before.
Meanwhile, nucleic acid tests by real-time RT-PCR assay were performed repeatedly. Nucleic acid tests were positive for five consecutive days from February 11 to 15. The results of the test on quarantine day 16 (February 26) turned negative, subsequently, on quarantine day 18 and 20, which were also negative. She was then released from quarantine on day 21 (March 2, 2020). Due to only laboratory-confirmed positive, case A was diagnosed as an asymptomatic carrier, manifested by Guangzhou Center for Disease Control and Prevention (GCDC).
2. Materials and methods
2.1. Study design and subjectsIn our study, asymptomatic COVID-19 carrier was defined as a patient without related clinical symptoms, but whose SARS-CoV-2 test was positive. Since Case A was diagnosed, all contacts, including hospital staffs, family members and patients, were routinely screened. Amounting to 455 contacts – 224 hospital staffs, 196 family members and 35 patients – who had been exposed to case A in EDOU or circulated area of it became the subjects of study.
Contacts were defined as individuals in the same ward with Case A. EDOU plus the circulated area of it covers 60 square meters where there are 14 patients’ beds placed at least 1.2 m apart. The study was approved by the Medical Ethical Committee of Guangdong Provincial People’s Hospital.
2.2. Data collectionIsolated individuals’ detailed information during the emergency department (ED) and hospitalization were retrospectively collected from electronic medical records, while other data were reviewed from documents recorded by related departments. Emphatically, we gathered their contact history, consisting of the date when they went to the emergency, the reason why they came to the emergency, and the time how long they were exposed to the case A. Demographics characteristics were also collected.
Any new symptoms on each person were taken down, both in ED and quarantine, including fever, cough, sputum production, sore throat, etc.
Meanwhile, we obtained imaging and laboratory data from hospital staffs and patients, which of family members were not noted. Each of patients had undergone a CT scan prior to admission because of the outbreak. It had been reviewed after the medical isolation began. Hospital staffs were examined one time. For laboratory test, a complete blood count was focus of attention. Nasopharyngeal swab specimens had been collected at least one time in whole people. All samples were processed at clinical laboratory of hospital and sent to GCDC simultaneously.
Patients and family members were quarantined for medical observation and hospital staffs were not quarantined because of standard protection, in principle.
2.3. Laboratory nucleic acid testIn accordance with the protocol announced previously by the WHO, RT-PCR can be considered in the assessment of individuals who have had contact with a COVID-19 case [13]. Consequently, whether the patients were infected with the SARS-CoV-2 was detected by real-time RT-PCR. Chinese Center for Disease Control and Prevention (CDC) published the sequences of primers and probe targeted to envelope gene of SARS-CoV-2, in January 21, 2020, which were as follows: forward primer 5′-TCAGAATGCCAATCTCCCCAAC-3′; reverse primer 5′-AAAGGTCCACCCGATACATTGA-3′; and probe 5′CY5CTAGTTACACTAGC-CATCCTTACTGC-3′BHQ1.
2.4. Statistical analysis
All research objects employed fundamental descriptive analysis. Continuous variables were expressed as the medians and interquartile ranges (IQR). Categorical variables in each category were summarized as counts and percentages. All statistical analyses were conducted with IBM SPSS statistics 24.0.
3. Results3.1. Patients
The statistics of 35 patients are displayed in Table 2 . All patients also wore masks except for eating or drinking and were admitted to infectious department for medical isolation. The median contact time was four days (interquartile range, 1.0 to 6.0), whereas the longest among them reached 21 days. The median age of the patients was 62 years (interquartile range, 50.0 to 84.0). A total of 57.1% were males. All individuals had been to ED of our hospital for various diseases. Undoubtedly, acute cardiovascular event and digestive diseases were common, accounting for 25.7% and 22.9%, respectively.
Table 2
Clinical characteristics of 35 patients.
CLINICAL CHARACTERISTICSPATIENTS (N = 35)Demographics characteristics
Age, median (IQR), years.
Male, sex, No. (%)62 (50.0–84.0)
20 (57.1)
Times of contact with Case A, median (IQR), days
Protopathy, No. (%)4 (1.0–6.0)
Cardiovascular disease9 (25.7)
Digestive diseases8 (22.9)
Cerebrovascular disease5 (14.3)
Orthopedic disease4 (11.4)
Hematological disease
Renal disease
Cancer2 (5.7)
2 (5.7)
3 (8.6)
Others12 (5.7)
Respiratory symptoms
None, No. (%)
Any, No. (%)
Fever
Newly emerged fever16 (45.7)
19 (54.3)
11 (31.4)
7 (20.0)
Cough8 (22.9)
Sputum4 (11.4)
Dyspnea7 (20.0)
Newly emerged dyspnea1 (2.9)
Laboratory findings
Leukocyte count ( × 109/L, normal range 4.0–10.0), No. (%)
Increased
Decreased
Normal14 (40.0)
3 (8.6)
18 (51.4)
Lymphocyte count ( × 109/L, normal range 1.5–3.5), No. (%)
Increased
Decreased
Normal1 (2.9)
12 (34.3)
22 (62.9)
Nucleic acid test negative, No. (%)35 (100.0)
Radiologic findings
Normal on chest CT, No. (%)11 (31.4)
Abnormalities on chest CT, No. (%)24 (68.6)
Inflammatory change12 (34.3)
Pleural effusion16 (45.7)
Interstitial change
Pulmonary edema2 (5.7)
1 (2.9)
Pulmonary nodule1 (2.9)
Clinical outcome
Transfer to specialized department, No. (%)25 (71.4)
Discharge from hospital, No. (%)8 (22.9)
Death, No. (%)2 (5.7)In terms of clinical symptoms, 16 (45.7%) patients were free of respiratory symptoms, which more than half of them (19 [54.3%]) appeared inversely. The respiratory symptoms involved fever (11 [31.4%]), cough (8 [22.9%]), dyspnea (7 [20.0%]) and sputum (4 [11.4%]). Among patients with fever, hyperthermia (body temperature >39 °C) occurred in one patient with chills after chemotherapy.
Three individuals presented slight fever (body temperature between 37.3 °C and 38.0 °C), of whom temperature could return to normal without therapy. Two individuals were diagnosed with infective endocarditis and acute pancreatitis severally with the cause of their symptoms including fever plus dyspnea and stomachache. Another five patients developed fever was consider as complication of the original disease, mostly pulmonary infection, whether the symptom was new or persistent. Last but not least, all dyspnea was associated with heart failure.
The blood counts in most patients were within normal range. Lymphocytopenia (<1.5 × 109 cells/L) had appeared in 34.3% of the patients and leukopenia (<4.0 × 109 cells/L) in 8.6%. One patient was also accompanied with neutropenia (<1.8 × 109 cells/L) on account of myelosuppression after chemotherapy. On the contrary, lymphocytosis (>3.5 × 109 cells/L) was observed in a patient with acute lymphoblastic leukemia. Besides one patient, died on quarantine 4-day,
34 patients underwent multiple nucleic acid tests of SARS-CoV-2. All the results were negative, including first time of the dead. Of 35 patients that had more than once chest CT scan, CT abnormalities were reported in 68.6%. The most common manifestations were inflammatory change (34.3%) and pleural effusion (45.7%). The interstitial change was detected less. Pulmonary edema and nodule were seen in persons with heart failure and lung cancer, respectively. Of particular concern, all CT findings were non-viral infection discussed professionally by radiologists. Normal CT image was found in 11 of 35 patients (31.4%).
According to evaluation from physicians, there were 19 infected patients (54.3%). Of these 19 patients, 15 (42.9%) had pneumonia, which was bacterial (37.1%), followed by pendulous (2.9%) and aspiration (2.9%). Mediastina inflammatory and abdominal infection arose from two patients with fistula. Other two patients had suffered from infection due to protopathy on admission. Above infected patients were administered for empirical antibiotic treatment. Four (11.4%) patients needed emergency surgery for their condition.
The rest of them (34.3%) were received to heteropathy.
It totally took 14 days from the last contact with Case A to the end of medical observation. As of Feb 26, 2020, none of 35 patients was diagnosed with SARS-CoV-2 infection. Among whom eight (22.9%) were discharged from the hospital while 25 (71.4%) were transferred to the specialized department for further treatments. The remaining two individuals both died for severe heart failure judged by the clinical expert panel during the period of quarantine.
3.2. Family membersIn total, 196 family members were enrolled. The situation on wearing masks was the same as that in patients. Local CDC took charge of following up 172 among them, who were ruled out SARS-CoV-2 infection after 14-days medical isolation, as far as we know. The rest of the escorts were placed in designated locations by GCDC for quarantine.
Of these 24 escorts, 11 were male and 13 were female. They aged from 24 to 86 years old and the median age was 47.5 years old (interquartile range, 34.0 to 57.0). The median contact time was five days (interquartile range, 1.0 to 11.0). Regarding examinations, at least two nucleic acid tests were negative. All the attendants except a family member had no respiratory symptoms in the time of quarantine. Details as below.
A 37-year-old woman, who had stayed in EDOU (February 7) for 10 h as relative, developed slight fever (the highest temperature was 37.5 °C), dry cough and sore throat after six days (February 13). Then she was presented to our hospital immediately. According to the investigation, she had worn a mask during the hospital visit and had a history of recurrent acute tonsillitis. After admission, her CT images and laboratory measurements were normal.
Additionally, she experienced four SARS-CoV-2 nucleic acid tests successively, all of which were negative. The case was given empirical antibiotic treatment since admission, and her symptoms disappeared afterwards. Based on clinical symptoms as well as auxiliary examination results, she received a diagnosis of acute tonsillitis finally. On Fberuray 25, she recovered and was discharged from the hospital.
3.3. Hospital staffsTo ensure safety, 224 hospital staffs who had come into contact with Case A were screened. As is clearly shown in Table 3 , their identities were mainly composed of doctors (59 [26.3%]) and nurses (101 [45.1%]). Others coexisted in the same room with Case A for work, such as security guards, cleaners, transportation personnel, etc. Of these 224 staffs, 103 were male and 121 were female, with ages ranging 21–60 years old.
The median age was 35 years old (interquartile range, 28.0 to 42.0). Most of them were emergency workers so that they had long exposure to confirmed case. Oppositely, some doctors in other departments had a brief stay, approximately one to 2 h, because of emergency consultation. It is noteworthy that all personnel working in ED must take medical protection – namely, using N95 mask, putting on isolation gown and wearing goggle.
Table 3
Clinical characteristics of 224 hospital staffs.
CLINICAL CHARACTERISTICSHOSPITAL STAFFS (N = 224)Demographics characteristics
Identity, No. (%)
Doctor59 (26.3)
Nurse101 (45.1)
Others164 (28.6)
Age, median (IQR), yr.
Male, sex, No. (%)35 (28.0–42.0)
103 (46.0)
Respiratory symptoms
None, No. (%)224 (100.0)
Laboratory findings
Leukocyte count ( × 109/L, normal range 4.0–10.0), No. (%)
Increased
Decreased
Normal29 (12.9)
0 (0.0)
195 (87.1)
Lymphocyte count ( × 109/L, normal range 1.5–3.5), No. (%)
Increased
Decreased
Normal5 (2.2)
3 (1.3)
216 (96.5)
Nucleic acid test negative, No. (%)224 (100.0)
Radiologic findings
Normal on chest CT, No./total No. (%)171/223 (76.7)
Abnormalities on chest CT, No./total No. (%)52/223 (23.3)
Pulmonary nodule29/223 (13.0)
Pulmonary fibrosis focus18/223 (8.1)
Pulmonary emphysema5/223 (2.2)
Quarantine personnel, No.
(%)0 (0.0)No respiratory symptoms were observed, either existing or emerging. Blood test results revealed normal leukocyte count in 87.1% and lymphocyte count in 96.5%. Lymphocyte counts were decreased in three staffs (1.3%) without leukopenia (<4.0 × 109 cells/L). A pregnant nurse failed to accept a CT scan. A minority of hospital staffs (52 [23.3%]) found abnormalities in CT, where pulmonary nodule, fibrosis focus and emphysema were seen. All hospital staffs were tested twice for SARS-CoV-2 nucleic acid, and the results were negative, which was identical with the two groups mentioned above. In contrast to them, none of 224 hospital staffs required medical observation.
4. DissusionIn this study, we recorded in detail the hospitalized situation, diagnostic procedure, inspection results, treatment plans and clinical outcome of an asymptomatic SARS-CoV-2 carrier who was laboratory confirmation by RT-PCR assay, but without related symptoms and imaging changes in concert with previous reports [12,14].
Also, we analyzed epidemiological and clinical data from 455 contacts who had been exposed to the asymptomatic patient. All the 455 contacts were excluded from SARS-CoV-2 infection. Of the 231 quarantined people (196 family members and 35 patients), 229 were removed from medical observation successfully and two died for severe heart failure. New or existing respiratory symptoms were almost appeared in patients, which were considered to be associated with their original disease or complications.
A family member complaining of fever was diagnosed as acute tonsillitis ultimately. Unlike COVID-19, normal blood count was found in most contacts [12,15]. All CT images showed no sign of COVID-19 infection. Unquestionably, all cases tested negative for SARS-CoV-2 nucleic acid. This fact illustrated that there had been no cases of infection in a relatively dense space.
Since the outbreak, our hospital has taken a series of effective prevention and control measures, which made a considerable effect on preventing the spread in this case. Above all, medical staffs abide by the principle of graded protection strictly. For patients and attendants, each patient can only be accompanied by one attendant, and both need to wear personal protective equipment (PPE). Nevertheless, there is still a risk of transmission of COVID-19 under stringent measures. Primarily, shortages of PPE were common in the early stages.
Medical resources were supplied to healthcare workers priorly. Due to these factors, patients and attendants can only wear one mask for a long time, resulting in its ineffective. Besides, we noticed that some patients and relatives wore PPE incorrectly due to the lack of adequate training, which was also possible for hospital staffs. Last but not least, it is unavoidable to take off mask while eating or drinking, which provides an opportunity to spread the virus.
Considering all the mentioned factors, we suggest that there are more important reasons for achieving “Zero infection”. As is well-known, person-to-person transmission through respiratory droplets is the main route of COVID-19 transmission [6].
Earlier research revealed that the viral load of respiratory tract samples in an asymptomatic patient was similar to that in the symptomatic patients [11]. However, a single sample is difficult to be representative. In the light of “Zero infection” for this case, we venture to guess that the viral load of respiratory tract samples in the asymptomatic patient might not be high.
Moreover, although pathogenic nucleic acids can be detected in respiratory tract samples from asymptomatic carriers, the opportunity of transmission is less than that in symptomatic patient owing to the absence of the way expelling pathogen via cough and sneezing.
Based on the foregoing discussion, we conclude that the infectivity of some asymptomatic SARS-CoV-2 carriers might be weak. This finding implicates that there is not needful to worry unduly for asymptomatic or mild patients during the ongoing COVID-19 pandemic. Furthermore, excessive virus nucleic acid detection is unnecessary, which can relieve the pressure on public health resources.
Under the development of epidemic circumstance, more and more public concerns on the increasing number of asymptomatic or mild patients hid in the community. However, combined with our results and the defense measures currently completed, we hope such worries are misplaced and we also believe the world will win this battle certainly.
The limitation of our study is that there is only one case and lack of detailed information on family members quarantined locally. Large-scale multicenter studies are needed to verify our conclusion. However, both asymptomatic carrier and 455 contacts were admitted to and treated in designated places. Hence, the study results are representative to some extent.
5. ConlusionsInfectivity of some asymptomatic SARS-CoV-2 carriers might be weak. Effective prevention and control measures are helpful to prevent COVID-19 spread of asymptomatic carriers. The result of this study may alleviate parts of the public concern about asymptomatic infected people.
FundingThis work was supported by the Science and Technology Planning Project of Guangdong Province (No. 2020B111111005).
CRediT authorship contribution statementMing Gao: Methodology, Data curation, Writing – original draft, Writing – review & editing. Lihui Yang: Investigation, Data curation, Formal analysis, Writing – review & editing. Xuefu Chen: Resources. Yiyu Deng: Writing – review & editing. Shifang Yang: Writing – review & editing. Hanyi Xu: Resources. Zixing Chen: Resources. Xinglin Gao: Conceptualization, Project administration, Supervision, Validation.
Declaration of competing interestThe authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
AcknowledgmentsWe owe thanks to the staffs of Guangdong Provincial People’s Hospital for gathering data in our study. We also acknowledge all the objects in this study and their family members.
Appendix A. Supplementary dataThe following is the Supplementary data to this article:
References1. Lescure F.X., Bouadma L., Nguyen D. Clinical and virological data of the first cases of COVID-19 in Europe: a case series. Lancet Infect. Dis. 2020 doi: 10.1016/S1473-3099(20)30200-0. Published Online March 27 2020. Available at: [CrossRef] [Google Scholar]
2. Adalja A.A., Toner E., Inglesby T.V. JAMA; 2020. Priorities for the US Health Community Responding to COVID-19. Published Online March 03 2020. Available at: [CrossRef] [Google Scholar]
3. McCloskey B., Zumla A., Ippolito G. Mass gathering events and reducing further global spread of COVID-19: a political and public health dilemma. Lancet. 2020;395:1096–1099. doi: 10.1016/S0140-6736(20)30681-4. Available at: [PMC free article] [PubMed] [CrossRef] [Google Scholar]
5. Lu R., Zhao X., Li J. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395:565–574. doi: 10.1016/S0140-6736(20)30251-8. Available at: [PMC free article] [PubMed] [CrossRef] [Google Scholar]
6. Wang Y., Wang Y., Yan Chen. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J. Med. Virol. 2020 doi: 10.1002/jmv.25748. Published Online March 05 2020. Available at: [CrossRef] [Google Scholar]
7. Del Rio C., Malani P.N. JAMA; 2020. COVID-19-New Insights on a Rapidly Changing Epidemic. Published Online February 28 2020. Available at: [CrossRef] [Google Scholar]
8. Zeng G., Xie S.Y., Li Q. Infectivity of severe acute respiratory syndrome during its incubation period. Biomed. Environ. Sci. 2009;22(6):502–510. doi: 10.1016/S0895-3988(10)60008-6. Available at: [PMC free article] [PubMed] [CrossRef] [Google Scholar]
10. Hu Z., Song C., Xu C. Life Sci; 2020. Clinical Characteristics of 24 Asymptomatic Infections with COVID-19 Screened Among Close Contacts in Nanjing, China. Sci China. Published Online March 04 2020. Available at: [CrossRef] [Google Scholar]
11. Zou L., Ruan F., Huang M. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N. Engl. J. Med. 2020;382:1177–1179. Available at: https://doi.org/10.1056/nejmc2001737. [PMC free article] [PubMed] [Google Scholar]
12. Guan W.J., Zhong N.S. Clinical characteristics of covid-19 in China. N. Engl. J. Med. 2020:382. [Google Scholar]
14. Salehi S., Abedi A., Balakrishnan S. Coronavirus disease 2019 (COVID-19): a systematic review of imaging findings in 919 patients. AJR Am. J. Roentgenol. 2020:1–7. doi: 10.2214/AJR.20.23034. Available at: [CrossRef] [Google Scholar]
15. Huang C., Wang Y., Li X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506. doi: 10.1016/S0140-6736(20)301847. Available at: [PMC free article] [PubMed] [CrossRef] [Google Scholar]
COVID-19, Coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; CHD, congenital heart disease; EDOU, emergency department observation unit; ED, emergency department; CT, computed tomography; RT-PCR, Reverse Transcription-Polymerase Chain Reaction; GCDC, Guangzhou Center for Disease Control and Prevention; CDC, Chinese Center for Disease Control and Prevention; IQR, interquartile ranges; PPE, personal protective equipment
1. Introdution
The emergence of the coronavirus disease 2019 (COVID-19) since early December 2019, has spread to many countries recently and sparked world pandemic via mass gathering [[1], [2], [3]]. As of March 24, 2020, there have been 334981 confirmed cases and 14652 deaths globally [4].
It has been proved that the pathogen of COVID-19 is severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which has high homology with SARS-CoV [5]. Similar to SARS-CoV, the dominant SARS-CoV-2 transmission mode is human-to-human transmission [6].
Differently, the reproductive number (R0) (the expected number of secondary cases produced by a single infected person in a susceptible population) is estimated between two and three, which is higher than SARS [6,7]. Furthermore, the transmission of SARS occurs during the symptomatic period [8]. For COVID-19, numerous asymptomatic infections were found among close contacts of confirmed patients, like the report on “Diamond Princess” [9].
However, the epidemiological significance of asymptomatic infections is unclear until now. Recent studies indicated that transmission of COVID-19 could also occur from these individuals with no symptoms [10,11]. However, for now, whether asymptomatic SARS-CoV-2 carriers are contagious still remain controversial.
Here, we report a case of an asymptomatic SARS-CoV-2 carrier with nosocomial infection and describe the clinical characteristics of 455 contacts. Our purpose is to analyze the infectivity of asymptomatic carriers.; CASE PRESENTATION.
Case A was a 22-year-old female patient who had a medical history of congenital heart disease (CHD) presented to the emergency room of Guangdong Provincial People’s Hospital (Guangzhou, Guangdong province, China) on January 13, 2020. She complained of shortness of breath for 16 years, and the symptom worsened for one month. The accompanied symptom was chest distress, without cough, sputum production and fever. Apart from CHD, she had no other diseases and had no smoking habit. Her temperature was normal, and laboratory measurements showed no apparent abnormalities (Table 1 ). Echocardiography displayed atrial septal defect and severe pulmonary hypertension. The diagnosis was congenital heart disease, atrial septal defect and pulmonary hypertension.
Table 1
Laboratory measurements of Case A.
JAN, 13FEB, 12FEB, 19FEB, 27NORMAL RANGEBlood count, × 10⁹/L
White blood cell count7.707.787.417.923.50–9.50
Neutrophil count4.974.144.164.441.80–6.30
Lymphocyte count2.132.912.132.631.10–3.20
Serological variables
C-reactive protein, mg/L0.65.89NTNT<5.0
Procalcitonin, ng/ml Normal NormalN TNT<0.05Case A was mainly given to oxygen therapy, diuretic treatment, plus pharmacotherapy of pulmonary hypertension. On January 16, as Case A’s condition improved and vital signs became stable, she was transferred to emergency department observation unit (EDOU). Owing to the Spring Festival and COVID-19 outbreak, she had been hospitalized in EDOU along with her brother until February 11.
Before admission, she underwent a serious of examinations according to hospital-formulated guidance during epidemic period. Nevertheless, the patient’s nasopharyngeal swab tested positive for SARS-CoV-2 by real-time Reverse Transcription-Polymerase Chain Reaction (RT-PCR). She was immediately admitted to quarantine ward in infectious department.
Case A and her brother both denied visiting Wuhan (the epidemic area in China) and any contact with COVID-19 patients. They wore masks all the time except at meals and drinking. How she became infected was unknown.
Notably, in isolation, the patient had never fever, sore throat, myalgia or other symptoms associated with virus infection [12]. Shortness of breath and chest distress, without further aggravation than before, were thought to be caused by CHD. Laboratory measurements reflected that white blood cells, lymphocytes, C-reactive protein and procalcitonin were within a normal range (Table 1).
Upon admission, chest computed tomography (CT) scan showed non- COVID-19 imaging feature (Fig. 1 . a, c). In the time of hospitalization, the patient received antiviral and interferon therapy. 11 days after the treatment (February 22), chest CT scan indicated no significant differences in comparison with before (Fig. 1. b, d).
Chest CT images of Case A.
Figure a and c were taken on February 11, which showed non- COVID-19 imaging feature. Case A underwent a CT scan again on February 22. Figure b and d, the follow-up images, showed no significant differences than before.
Meanwhile, nucleic acid tests by real-time RT-PCR assay were performed repeatedly. Nucleic acid tests were positive for five consecutive days from February 11 to 15. The results of the test on quarantine day 16 (February 26) turned negative, subsequently, on quarantine day 18 and 20, which were also negative. She was then released from quarantine on day 21 (March 2, 2020). Due to only laboratory-confirmed positive, case A was diagnosed as an asymptomatic carrier, manifested by Guangzhou Center for Disease Control and Prevention (GCDC).
2. Materials and methods
2.1. Study design and subjectsIn our study, asymptomatic COVID-19 carrier was defined as a patient without related clinical symptoms, but whose SARS-CoV-2 test was positive. Since Case A was diagnosed, all contacts, including hospital staffs, family members and patients, were routinely screened. Amounting to 455 contacts – 224 hospital staffs, 196 family members and 35 patients – who had been exposed to case A in EDOU or circulated area of it became the subjects of study.
Contacts were defined as individuals in the same ward with Case A. EDOU plus the circulated area of it covers 60 square meters where there are 14 patients’ beds placed at least 1.2 m apart. The study was approved by the Medical Ethical Committee of Guangdong Provincial People’s Hospital.
2.2. Data collectionIsolated individuals’ detailed information during the emergency department (ED) and hospitalization were retrospectively collected from electronic medical records, while other data were reviewed from documents recorded by related departments. Emphatically, we gathered their contact history, consisting of the date when they went to the emergency, the reason why they came to the emergency, and the time how long they were exposed to the case A. Demographics characteristics were also collected.
Any new symptoms on each person were taken down, both in ED and quarantine, including fever, cough, sputum production, sore throat, etc.
Meanwhile, we obtained imaging and laboratory data from hospital staffs and patients, which of family members were not noted. Each of patients had undergone a CT scan prior to admission because of the outbreak. It had been reviewed after the medical isolation began. Hospital staffs were examined one time. For laboratory test, a complete blood count was focus of attention. Nasopharyngeal swab specimens had been collected at least one time in whole people. All samples were processed at clinical laboratory of hospital and sent to GCDC simultaneously.
Patients and family members were quarantined for medical observation and hospital staffs were not quarantined because of standard protection, in principle.
2.3. Laboratory nucleic acid testIn accordance with the protocol announced previously by the WHO, RT-PCR can be considered in the assessment of individuals who have had contact with a COVID-19 case [13]. Consequently, whether the patients were infected with the SARS-CoV-2 was detected by real-time RT-PCR. Chinese Center for Disease Control and Prevention (CDC) published the sequences of primers and probe targeted to envelope gene of SARS-CoV-2, in January 21, 2020, which were as follows: forward primer 5′-TCAGAATGCCAATCTCCCCAAC-3′; reverse primer 5′-AAAGGTCCACCCGATACATTGA-3′; and probe 5′CY5CTAGTTACACTAGC-CATCCTTACTGC-3′BHQ1.
2.4. Statistical analysis
All research objects employed fundamental descriptive analysis. Continuous variables were expressed as the medians and interquartile ranges (IQR). Categorical variables in each category were summarized as counts and percentages. All statistical analyses were conducted with IBM SPSS statistics 24.0.
3. Results3.1. Patients
The statistics of 35 patients are displayed in Table 2 . All patients also wore masks except for eating or drinking and were admitted to infectious department for medical isolation. The median contact time was four days (interquartile range, 1.0 to 6.0), whereas the longest among them reached 21 days. The median age of the patients was 62 years (interquartile range, 50.0 to 84.0). A total of 57.1% were males. All individuals had been to ED of our hospital for various diseases. Undoubtedly, acute cardiovascular event and digestive diseases were common, accounting for 25.7% and 22.9%, respectively.
Table 2
Clinical characteristics of 35 patients.
CLINICAL CHARACTERISTICSPATIENTS (N = 35)Demographics characteristics
Age, median (IQR), years.
Male, sex, No. (%)62 (50.0–84.0)
20 (57.1)
Times of contact with Case A, median (IQR), days
Protopathy, No. (%)4 (1.0–6.0)
Cardiovascular disease9 (25.7)
Digestive diseases8 (22.9)
Cerebrovascular disease5 (14.3)
Orthopedic disease4 (11.4)
Hematological disease
Renal disease
Cancer2 (5.7)
2 (5.7)
3 (8.6)
Others12 (5.7)
Respiratory symptoms
None, No. (%)
Any, No. (%)
Fever
Newly emerged fever16 (45.7)
19 (54.3)
11 (31.4)
7 (20.0)
Cough8 (22.9)
Sputum4 (11.4)
Dyspnea7 (20.0)
Newly emerged dyspnea1 (2.9)
Laboratory findings
Leukocyte count ( × 109/L, normal range 4.0–10.0), No. (%)
Increased
Decreased
Normal14 (40.0)
3 (8.6)
18 (51.4)
Lymphocyte count ( × 109/L, normal range 1.5–3.5), No. (%)
Increased
Decreased
Normal1 (2.9)
12 (34.3)
22 (62.9)
Nucleic acid test negative, No. (%)35 (100.0)
Radiologic findings
Normal on chest CT, No. (%)11 (31.4)
Abnormalities on chest CT, No. (%)24 (68.6)
Inflammatory change12 (34.3)
Pleural effusion16 (45.7)
Interstitial change
Pulmonary edema2 (5.7)
1 (2.9)
Pulmonary nodule1 (2.9)
Clinical outcome
Transfer to specialized department, No. (%)25 (71.4)
Discharge from hospital, No. (%)8 (22.9)
Death, No. (%)2 (5.7)In terms of clinical symptoms, 16 (45.7%) patients were free of respiratory symptoms, which more than half of them (19 [54.3%]) appeared inversely. The respiratory symptoms involved fever (11 [31.4%]), cough (8 [22.9%]), dyspnea (7 [20.0%]) and sputum (4 [11.4%]). Among patients with fever, hyperthermia (body temperature >39 °C) occurred in one patient with chills after chemotherapy.
Three individuals presented slight fever (body temperature between 37.3 °C and 38.0 °C), of whom temperature could return to normal without therapy. Two individuals were diagnosed with infective endocarditis and acute pancreatitis severally with the cause of their symptoms including fever plus dyspnea and stomachache. Another five patients developed fever was consider as complication of the original disease, mostly pulmonary infection, whether the symptom was new or persistent. Last but not least, all dyspnea was associated with heart failure.
The blood counts in most patients were within normal range. Lymphocytopenia (<1.5 × 109 cells/L) had appeared in 34.3% of the patients and leukopenia (<4.0 × 109 cells/L) in 8.6%. One patient was also accompanied with neutropenia (<1.8 × 109 cells/L) on account of myelosuppression after chemotherapy. On the contrary, lymphocytosis (>3.5 × 109 cells/L) was observed in a patient with acute lymphoblastic leukemia. Besides one patient, died on quarantine 4-day,
34 patients underwent multiple nucleic acid tests of SARS-CoV-2. All the results were negative, including first time of the dead. Of 35 patients that had more than once chest CT scan, CT abnormalities were reported in 68.6%. The most common manifestations were inflammatory change (34.3%) and pleural effusion (45.7%). The interstitial change was detected less. Pulmonary edema and nodule were seen in persons with heart failure and lung cancer, respectively. Of particular concern, all CT findings were non-viral infection discussed professionally by radiologists. Normal CT image was found in 11 of 35 patients (31.4%).
According to evaluation from physicians, there were 19 infected patients (54.3%). Of these 19 patients, 15 (42.9%) had pneumonia, which was bacterial (37.1%), followed by pendulous (2.9%) and aspiration (2.9%). Mediastina inflammatory and abdominal infection arose from two patients with fistula. Other two patients had suffered from infection due to protopathy on admission. Above infected patients were administered for empirical antibiotic treatment. Four (11.4%) patients needed emergency surgery for their condition.
The rest of them (34.3%) were received to heteropathy.
It totally took 14 days from the last contact with Case A to the end of medical observation. As of Feb 26, 2020, none of 35 patients was diagnosed with SARS-CoV-2 infection. Among whom eight (22.9%) were discharged from the hospital while 25 (71.4%) were transferred to the specialized department for further treatments. The remaining two individuals both died for severe heart failure judged by the clinical expert panel during the period of quarantine.
3.2. Family membersIn total, 196 family members were enrolled. The situation on wearing masks was the same as that in patients. Local CDC took charge of following up 172 among them, who were ruled out SARS-CoV-2 infection after 14-days medical isolation, as far as we know. The rest of the escorts were placed in designated locations by GCDC for quarantine.
Of these 24 escorts, 11 were male and 13 were female. They aged from 24 to 86 years old and the median age was 47.5 years old (interquartile range, 34.0 to 57.0). The median contact time was five days (interquartile range, 1.0 to 11.0). Regarding examinations, at least two nucleic acid tests were negative. All the attendants except a family member had no respiratory symptoms in the time of quarantine. Details as below.
A 37-year-old woman, who had stayed in EDOU (February 7) for 10 h as relative, developed slight fever (the highest temperature was 37.5 °C), dry cough and sore throat after six days (February 13). Then she was presented to our hospital immediately. According to the investigation, she had worn a mask during the hospital visit and had a history of recurrent acute tonsillitis. After admission, her CT images and laboratory measurements were normal.
Additionally, she experienced four SARS-CoV-2 nucleic acid tests successively, all of which were negative. The case was given empirical antibiotic treatment since admission, and her symptoms disappeared afterwards. Based on clinical symptoms as well as auxiliary examination results, she received a diagnosis of acute tonsillitis finally. On Fberuray 25, she recovered and was discharged from the hospital.
3.3. Hospital staffsTo ensure safety, 224 hospital staffs who had come into contact with Case A were screened. As is clearly shown in Table 3 , their identities were mainly composed of doctors (59 [26.3%]) and nurses (101 [45.1%]). Others coexisted in the same room with Case A for work, such as security guards, cleaners, transportation personnel, etc. Of these 224 staffs, 103 were male and 121 were female, with ages ranging 21–60 years old.
The median age was 35 years old (interquartile range, 28.0 to 42.0). Most of them were emergency workers so that they had long exposure to confirmed case. Oppositely, some doctors in other departments had a brief stay, approximately one to 2 h, because of emergency consultation. It is noteworthy that all personnel working in ED must take medical protection – namely, using N95 mask, putting on isolation gown and wearing goggle.
Table 3
Clinical characteristics of 224 hospital staffs.
CLINICAL CHARACTERISTICSHOSPITAL STAFFS (N = 224)Demographics characteristics
Identity, No. (%)
Doctor59 (26.3)
Nurse101 (45.1)
Others164 (28.6)
Age, median (IQR), yr.
Male, sex, No. (%)35 (28.0–42.0)
103 (46.0)
Respiratory symptoms
None, No. (%)224 (100.0)
Laboratory findings
Leukocyte count ( × 109/L, normal range 4.0–10.0), No. (%)
Increased
Decreased
Normal29 (12.9)
0 (0.0)
195 (87.1)
Lymphocyte count ( × 109/L, normal range 1.5–3.5), No. (%)
Increased
Decreased
Normal5 (2.2)
3 (1.3)
216 (96.5)
Nucleic acid test negative, No. (%)224 (100.0)
Radiologic findings
Normal on chest CT, No./total No. (%)171/223 (76.7)
Abnormalities on chest CT, No./total No. (%)52/223 (23.3)
Pulmonary nodule29/223 (13.0)
Pulmonary fibrosis focus18/223 (8.1)
Pulmonary emphysema5/223 (2.2)
Quarantine personnel, No.
(%)0 (0.0)No respiratory symptoms were observed, either existing or emerging. Blood test results revealed normal leukocyte count in 87.1% and lymphocyte count in 96.5%. Lymphocyte counts were decreased in three staffs (1.3%) without leukopenia (<4.0 × 109 cells/L). A pregnant nurse failed to accept a CT scan. A minority of hospital staffs (52 [23.3%]) found abnormalities in CT, where pulmonary nodule, fibrosis focus and emphysema were seen. All hospital staffs were tested twice for SARS-CoV-2 nucleic acid, and the results were negative, which was identical with the two groups mentioned above. In contrast to them, none of 224 hospital staffs required medical observation.
4. DissusionIn this study, we recorded in detail the hospitalized situation, diagnostic procedure, inspection results, treatment plans and clinical outcome of an asymptomatic SARS-CoV-2 carrier who was laboratory confirmation by RT-PCR assay, but without related symptoms and imaging changes in concert with previous reports [12,14].
Also, we analyzed epidemiological and clinical data from 455 contacts who had been exposed to the asymptomatic patient. All the 455 contacts were excluded from SARS-CoV-2 infection. Of the 231 quarantined people (196 family members and 35 patients), 229 were removed from medical observation successfully and two died for severe heart failure. New or existing respiratory symptoms were almost appeared in patients, which were considered to be associated with their original disease or complications.
A family member complaining of fever was diagnosed as acute tonsillitis ultimately. Unlike COVID-19, normal blood count was found in most contacts [12,15]. All CT images showed no sign of COVID-19 infection. Unquestionably, all cases tested negative for SARS-CoV-2 nucleic acid. This fact illustrated that there had been no cases of infection in a relatively dense space.
Since the outbreak, our hospital has taken a series of effective prevention and control measures, which made a considerable effect on preventing the spread in this case. Above all, medical staffs abide by the principle of graded protection strictly. For patients and attendants, each patient can only be accompanied by one attendant, and both need to wear personal protective equipment (PPE). Nevertheless, there is still a risk of transmission of COVID-19 under stringent measures. Primarily, shortages of PPE were common in the early stages.
Medical resources were supplied to healthcare workers priorly. Due to these factors, patients and attendants can only wear one mask for a long time, resulting in its ineffective. Besides, we noticed that some patients and relatives wore PPE incorrectly due to the lack of adequate training, which was also possible for hospital staffs. Last but not least, it is unavoidable to take off mask while eating or drinking, which provides an opportunity to spread the virus.
Considering all the mentioned factors, we suggest that there are more important reasons for achieving “Zero infection”. As is well-known, person-to-person transmission through respiratory droplets is the main route of COVID-19 transmission [6].
Earlier research revealed that the viral load of respiratory tract samples in an asymptomatic patient was similar to that in the symptomatic patients [11]. However, a single sample is difficult to be representative. In the light of “Zero infection” for this case, we venture to guess that the viral load of respiratory tract samples in the asymptomatic patient might not be high.
Moreover, although pathogenic nucleic acids can be detected in respiratory tract samples from asymptomatic carriers, the opportunity of transmission is less than that in symptomatic patient owing to the absence of the way expelling pathogen via cough and sneezing.
Based on the foregoing discussion, we conclude that the infectivity of some asymptomatic SARS-CoV-2 carriers might be weak. This finding implicates that there is not needful to worry unduly for asymptomatic or mild patients during the ongoing COVID-19 pandemic. Furthermore, excessive virus nucleic acid detection is unnecessary, which can relieve the pressure on public health resources.
Under the development of epidemic circumstance, more and more public concerns on the increasing number of asymptomatic or mild patients hid in the community. However, combined with our results and the defense measures currently completed, we hope such worries are misplaced and we also believe the world will win this battle certainly.
The limitation of our study is that there is only one case and lack of detailed information on family members quarantined locally. Large-scale multicenter studies are needed to verify our conclusion. However, both asymptomatic carrier and 455 contacts were admitted to and treated in designated places. Hence, the study results are representative to some extent.
5. ConlusionsInfectivity of some asymptomatic SARS-CoV-2 carriers might be weak. Effective prevention and control measures are helpful to prevent COVID-19 spread of asymptomatic carriers. The result of this study may alleviate parts of the public concern about asymptomatic infected people.
FundingThis work was supported by the Science and Technology Planning Project of Guangdong Province (No. 2020B111111005).
CRediT authorship contribution statementMing Gao: Methodology, Data curation, Writing – original draft, Writing – review & editing. Lihui Yang: Investigation, Data curation, Formal analysis, Writing – review & editing. Xuefu Chen: Resources. Yiyu Deng: Writing – review & editing. Shifang Yang: Writing – review & editing. Hanyi Xu: Resources. Zixing Chen: Resources. Xinglin Gao: Conceptualization, Project administration, Supervision, Validation.
Declaration of competing interestThe authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
AcknowledgmentsWe owe thanks to the staffs of Guangdong Provincial People’s Hospital for gathering data in our study. We also acknowledge all the objects in this study and their family members.
Appendix A. Supplementary dataThe following is the Supplementary data to this article:
References1. Lescure F.X., Bouadma L., Nguyen D. Clinical and virological data of the first cases of COVID-19 in Europe: a case series. Lancet Infect. Dis. 2020 doi: 10.1016/S1473-3099(20)30200-0. Published Online March 27 2020. Available at: [CrossRef] [Google Scholar]
2. Adalja A.A., Toner E., Inglesby T.V. JAMA; 2020. Priorities for the US Health Community Responding to COVID-19. Published Online March 03 2020. Available at: [CrossRef] [Google Scholar]
3. McCloskey B., Zumla A., Ippolito G. Mass gathering events and reducing further global spread of COVID-19: a political and public health dilemma. Lancet. 2020;395:1096–1099. doi: 10.1016/S0140-6736(20)30681-4. Available at: [PMC free article] [PubMed] [CrossRef] [Google Scholar]
5. Lu R., Zhao X., Li J. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395:565–574. doi: 10.1016/S0140-6736(20)30251-8. Available at: [PMC free article] [PubMed] [CrossRef] [Google Scholar]
6. Wang Y., Wang Y., Yan Chen. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J. Med. Virol. 2020 doi: 10.1002/jmv.25748. Published Online March 05 2020. Available at: [CrossRef] [Google Scholar]
7. Del Rio C., Malani P.N. JAMA; 2020. COVID-19-New Insights on a Rapidly Changing Epidemic. Published Online February 28 2020. Available at: [CrossRef] [Google Scholar]
8. Zeng G., Xie S.Y., Li Q. Infectivity of severe acute respiratory syndrome during its incubation period. Biomed. Environ. Sci. 2009;22(6):502–510. doi: 10.1016/S0895-3988(10)60008-6. Available at: [PMC free article] [PubMed] [CrossRef] [Google Scholar]
10. Hu Z., Song C., Xu C. Life Sci; 2020. Clinical Characteristics of 24 Asymptomatic Infections with COVID-19 Screened Among Close Contacts in Nanjing, China. Sci China. Published Online March 04 2020. Available at: [CrossRef] [Google Scholar]
11. Zou L., Ruan F., Huang M. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N. Engl. J. Med. 2020;382:1177–1179. Available at: https://doi.org/10.1056/nejmc2001737. [PMC free article] [PubMed] [Google Scholar]
12. Guan W.J., Zhong N.S. Clinical characteristics of covid-19 in China. N. Engl. J. Med. 2020:382. [Google Scholar]
14. Salehi S., Abedi A., Balakrishnan S. Coronavirus disease 2019 (COVID-19): a systematic review of imaging findings in 919 patients. AJR Am. J. Roentgenol. 2020:1–7. doi: 10.2214/AJR.20.23034. Available at: [CrossRef] [Google Scholar]
15. Huang C., Wang Y., Li X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506. doi: 10.1016/S0140-6736(20)301847. Available at: [PMC free article] [PubMed] [CrossRef] [Google Scholar]
- Pingback: Watch under a Microscope – Your cells create a Corona Cell…Have we been Conned into Killing Our Immune System? | Health and Money News
- Pingback: Face Masks Pose Serious Risks To The Healthy – Dr. Blaylock- Neurosurgeon | Health and Money News
- Pingback: The Economic “Reopening” Is A Fake Out | Health and Money News
- Pingback: Your New UN Passport to Work, Travel, & Survive – The Covi-Pass — VACCINE Passport to Complete Slavery | Health and Money News
- Pingback: MIT: A Nation Where Half of the Children Become Autistic? | Health and Money News
- Pingback: New World Order Now Has a New Web Site– for the HAPPY TOTAL ENSLAVEMENT FOR ALL | Health and Money News
- Pingback: I Wear My Face Mask in the Car | Health and Money News
- Pingback: Vaccine Companies Can Damage or Kill You With Complete Immunity | Health and Money News
- Pingback: You are now a Lab Rat…Masks & Social Distancing are Illegal– Now You Can Do Something About It! | Health and Money News
- Pingback: Many will die from this “Mandatory” Vaccine | Health and Money News
- Pingback: It Will Be Mandatory? Something Major is Happening | Health and Money News
- Pingback: A Letter From A Friend-COVID-19 IS NOT A VIRUS | Health and Money News
- Pingback: Polio Vaccine Caused 70,000 Cases of Polio in US Alone | Health and Money News
- Pingback: What Polio Vaccine Injury Looks Like, Decades Later | Health and Money News
- Pingback: The Injection Fraud – It’s Not a Vaccine | Health and Money News
- Pingback: CDC Admits Covid-19 No Worse Than Yearly Flu & Tests Are A Waste of Time | Health and Money News
- Pingback: SIMON SAYS? – The WHO Now Recommends Not To Wear Masks | Health and Money News
- Pingback: One in Every 16 Irish Boys has Autism: Crisis Worse than COVID-19 and Nobody Cares | Health and Money News
- Pingback: German Government: Entire Corona is “A Global False Alarm” | Health and Money News
- Pingback: Constitutional Attorney Eviscerates Dershowitz’s Claim of Constitutionality Of Forced Mandatory Vaccination | Health and Money News
- Pingback: Merck Rep Says Mandatory Vaccination Is For Profit, Toxic, and Not For Public Health | Health and Money News
- Pingback: Flue Shot Bombshell: Flu Shot More Deadly than Covid-19- According To Vaccine Manufacturer ! | Health and Money News
- Pingback: Why The Public Should Rebel Against Forced Vaccinations | Health and Money News
- Pingback: ‘Absolutely no evidence’ that COVID-19 is airborne, B.C. health official says | Health and Money News
- Pingback: Do You Know What’s In A Vaccine? | Health and Money News
- Pingback: Enraged Italians Abandon Masks, Denounce Pandemic As Scam | Health and Money News
- Pingback: Fox News: Bill Gates Paid The World Health Organization $50 Million to Declare a Pandemic | Health and Money News
🌸
Fox News:
Bill Gates Paid The World Health Organization
$50 Million to Declare a Pandemic
🌸
Around the 3 minute mark: “WHO didn’t want to declare Covid19 as a pandemic –
a day later Bill Gates infused 50 million dollars towards WHO – one day later the
WHO secretary general declared it a pandemic”
When are people going to understand that Bill Gates and others in the deep state
want to depopulate the world to under 500,000,000.
To do this 95% of the world’s population must die.
Gates makes no excuses, this is what he is striving for ...
he says vaccines will help to depopulate and make others infertile.
Fox News:
Bill Gates Paid The World Health Organization
$50 Million to Declare a Pandemic
🌸
Around the 3 minute mark: “WHO didn’t want to declare Covid19 as a pandemic –
a day later Bill Gates infused 50 million dollars towards WHO – one day later the
WHO secretary general declared it a pandemic”
When are people going to understand that Bill Gates and others in the deep state
want to depopulate the world to under 500,000,000.
To do this 95% of the world’s population must die.
Gates makes no excuses, this is what he is striving for ...
he says vaccines will help to depopulate and make others infertile.
🌸
Coronavirus
(disambiguation)
The virus is only active during certain times of the day.
It also can travel up to 6 feet, but cannot travel 6’ 1” or greater.
It can go through the air and all surfaces,
except anything that comes in the mail or groceries you take home.
The virus doesn’t go to places like Walmart, Target, Amazon
or other large corporations and grocery stores,
but it likes bars, small businesses and especially churches
where it can travel up to 9 feet.
The virus live on food taken to - go, because it stays inside restaurants.
All are very confusing, but it is the Modern Science.
🌸
(disambiguation)
The virus is only active during certain times of the day.
It also can travel up to 6 feet, but cannot travel 6’ 1” or greater.
It can go through the air and all surfaces,
except anything that comes in the mail or groceries you take home.
The virus doesn’t go to places like Walmart, Target, Amazon
or other large corporations and grocery stores,
but it likes bars, small businesses and especially churches
where it can travel up to 9 feet.
The virus live on food taken to - go, because it stays inside restaurants.
All are very confusing, but it is the Modern Science.
🌸
Have We Been Conned
Into Killing Our Immune System?
🌸
Into Killing Our Immune System?
🌸