✴︎
Caution in Identifying Coronaviruses
by Electron Microscopy
✴︎
Electron microscope images of the COVID-19 coronavirus have been brought into question.
✴︎
Caution in Identifying Coronaviruses
by Electron Microscopy
✴︎
Electron microscope images of the COVID-19 coronavirus have been brought into question.
✴︎
✴︎
Have Any Human Coronaviruses Been Isolated?
✴︎
It Has Been Confirmed: PCR Does Not Detect SARS-CoV-2
✴︎
GreenMedInfo.
Have Any Human Coronaviruses Been Isolated?
✴︎
It Has Been Confirmed: PCR Does Not Detect SARS-CoV-2
✴︎
GreenMedInfo.
✴︎
Does the COVID-19 coronavirus even exist?
✴︎
www.lewrockwell.com/2020/12/no_author/survey-confirms-were-killing-ourselves-its-a-lifestyle-dietary-disease-vaccines-wont-help/
✴︎
While graphic images of the COVID-19 coronavirus show outward facing spikes, electron microscope images show these spikes face inwards in living cells.
It is easy to misinterpret other intracellular structures as coronavirus particles.
The news media has largely used fake images of COVID-19 coronavirus.
Neither does the current Polymerase Chain Reaction-PCR test reliably detect COVID-19.
So, does COVID-19 really exist?
✴︎
A thorough analysis of the test to detect COVID-19 coronavirus infection was conducted
by Jesus Garcia Blanca
(Discovery Health, November 2020).
The original version of this report is in Spanish language
but is reproduced in English
at GreenMedInfo.
Dr. Blanca’s study reveals the genetic sequences (DNA letters)
used in the polymerase chain reaction (PCR) test are present in the human genome itself and therefore the PCR test is worthless.
The original sequence of COVID-19 virus corresponds to 74 sequences in the human genome,
so it is not a novel mutation.
To date, a purified virus has not been produced to serve as a standard.
The PCR test only detects fragments of human RNA, not COVID-19 in its entirety.
None of the seven known
coronaviruses have been isolated and characterized either.
All of the RNA sequences for COVID-19 have been found in other bacteria.
One effort to isolate a coronavirus admits researchers
“manually assembled and edited to produce a final sequence of the viral genome.”
Therefore, no coronavirus can be held responsible for any disease.
Maybe this is why no vaccine against any coronavirus has been licensed in the past decade.
Numerous inquiries into confirmation of the COVID-19 coronavirus
at university databases have resulted in the same answer:
“No record of work describing the isolation of the virus that is supposed
to cause COVID19 can be found.”
Does the COVID-19 coronavirus even exist?
✴︎
www.lewrockwell.com/2020/12/no_author/survey-confirms-were-killing-ourselves-its-a-lifestyle-dietary-disease-vaccines-wont-help/
✴︎
While graphic images of the COVID-19 coronavirus show outward facing spikes, electron microscope images show these spikes face inwards in living cells.
It is easy to misinterpret other intracellular structures as coronavirus particles.
The news media has largely used fake images of COVID-19 coronavirus.
Neither does the current Polymerase Chain Reaction-PCR test reliably detect COVID-19.
So, does COVID-19 really exist?
✴︎
A thorough analysis of the test to detect COVID-19 coronavirus infection was conducted
by Jesus Garcia Blanca
(Discovery Health, November 2020).
The original version of this report is in Spanish language
but is reproduced in English
at GreenMedInfo.
Dr. Blanca’s study reveals the genetic sequences (DNA letters)
used in the polymerase chain reaction (PCR) test are present in the human genome itself and therefore the PCR test is worthless.
The original sequence of COVID-19 virus corresponds to 74 sequences in the human genome,
so it is not a novel mutation.
To date, a purified virus has not been produced to serve as a standard.
The PCR test only detects fragments of human RNA, not COVID-19 in its entirety.
None of the seven known
coronaviruses have been isolated and characterized either.
All of the RNA sequences for COVID-19 have been found in other bacteria.
One effort to isolate a coronavirus admits researchers
“manually assembled and edited to produce a final sequence of the viral genome.”
Therefore, no coronavirus can be held responsible for any disease.
Maybe this is why no vaccine against any coronavirus has been licensed in the past decade.
Numerous inquiries into confirmation of the COVID-19 coronavirus
at university databases have resulted in the same answer:
“No record of work describing the isolation of the virus that is supposed
to cause COVID19 can be found.”
✴︎

✴︎
Survey Confirms:
✴︎
We’re Killing Ourselves It’s A Lifestyle Dietary Disease
Vaccines Won’t Help
✴︎
Death by Alcohol, Sugar, Coffee & Tea
Binging Results in A B-Vitamin Deficiency
and Loss of Control of the Nervous System
By Bill Sardi
✴︎
✴︎
We’re Killing Ourselves It’s A Lifestyle Dietary Disease
Vaccines Won’t Help
✴︎
Death by Alcohol, Sugar, Coffee & Tea
Binging Results in A B-Vitamin Deficiency
and Loss of Control of the Nervous System
By Bill Sardi
✴︎
December 19, 2020
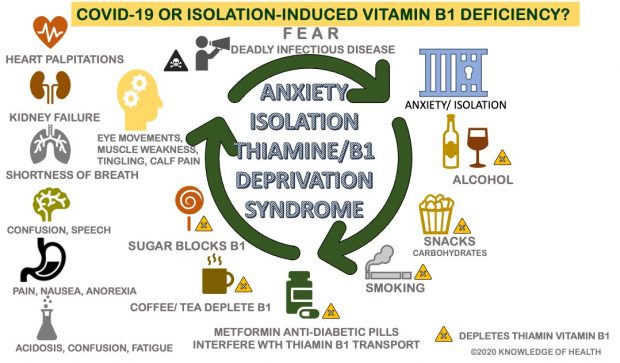
Since the inception of the COVID-19 lockdown measures, human populations have been suffering with an anxiety-induced syndrome that has increased an already prevalent B-vitamin deficiency, a nutrient that controls the autonomic nervous system that unconsciously controls heartbeat, breathing, digestion, and all the senses of smell, taste, touch and hearing.
The fear-evoking idea that a mutated cold-virus against which humanity had no immunity towards could swiftly induce breathlessness and take someone’s life away is something human populations of the world certainly can’t get off their minds. With no proven treatments or vaccines, the world is gripped with fear. The Grim Reaper delivers death even among seemingly healthy individuals. Who will be next?
But erase the COVID-19 case and death scoreboard and the fear that accompanies it. It’s all a ruse, a mass deception. Yes, people are dying, but not from a mutated coronavirus, or any coronavirus for that matter. The “co-morbidities” that accompany COVID-19, diabetes, heart disease, blood coagulation, kidney failure, are more likely the result of a change in dietary practices during lockdown than any imagined coronavirus.
We’re killing ourselves by eating and drinking ourselves to death
The lockdowns were predicted to generate 29-times more deaths than from the coronavirus itself.
Why?
What is causing many adults to die of breathlessness in hospital ICUs?
Results from a recent survey conducted by OnePoll market research, on behalf of a canned drinking water brand that adds hops and other “adaptogens” as a healthy alternative to beer, reveals COVID-19 is a lifestyle disease that brings on an anxiety-induced dietary and beverage changes.
The polling organization doesn’t realize all these changes in dietary practices block an essential nutrient needed for nervous system control.
The OnePoll survey reveals Americans are drinking more alcohol at home, consuming more “comfort foods” and swallowing down more coffee and tea to deal with fatigue and sleep loss.
The survey reveals 46% of those Americans working at home pour themselves an alcoholic drink during the workday; 53% of Americans are drinking more frequently during the lockdown.
Of particular interest is a survey which shows 52% of respondents felt a need to drink while watching the news on TV.
According to the National Institute on Alcohol Abuse & Alcoholism, there are 14.1 million American adults who have “alcohol use disorder.” Vitamin B1 deficiency is common among alcohol imbibers.
Two-in-five say also say they have been snacking more, and consuming “comfort foods.” That translates to “carbohydrates,” bread/pastry, rice, pasta, cereal.
Add 32% who claim they are drinking too much caffeinated beverages – – coffee and tea.
All of these anxiety/fatigue related foods and beverages interfere with vitamin B1 nutriture.
What started in Wuhan, China is not the COVID-19 of today
The COVID-19 coronavirus that started this worldwide pandemic in late 2019 is not the COVID-19 syndrome the public faces today during the lockdown era of the disease.
Bear with me a moment as I digress back to the start of the COVID-19 coronavirus outbreak. COVID-19 may have initially been panned as emanating from a mutated virus in Wuhan, China, where health authorities had been battling an outbreak of tuberculosis two years prior to COVID-19.
TB is, like COVID-19, a seasonal infectious lung disease, not caused by a virus but rather a mycobacterium.
TB could easily have been re-categorized as a COVID-19 coronavirus infection. Modena, Italy and New York City, two other COVID-19 geographic hotspots, were also plagued by prior TB outbreaks.
The Bacillus Calmette Guerin TB vaccine protects against COVID-19 infection, which also suggests TB cases were simply re-categorized as COVID-19. Oddly, nobody has raised suspicion that COVID-19 may simply be TB.
And what happened to Wuhan? There are barely any new cases in that city of 11 million people, while the US reports all-time high death counts.
Then came the lockdowns and what appeared to be a second round of COVID-19 that was in fact caused by the lockdowns themselves.
Loss of nervous system control
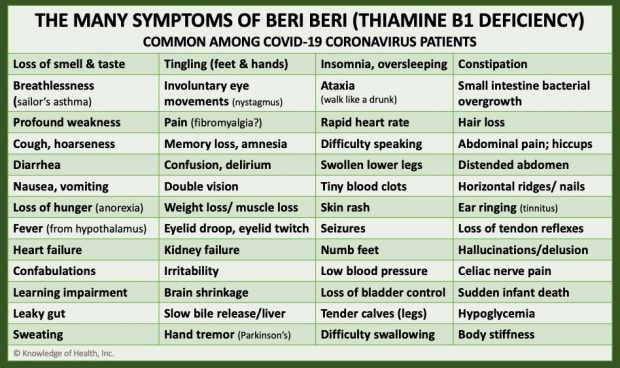
Vitamin B1 controls the autonomic nervous system – – heartbeat, breathing, digestion and elimination, and all the senses (touch/pain, smell, taste, hearing, vision). The chronic symptoms that characterize “long-haul” COVID – – headaches, crushing fatigue, loss of memory, weak muscles, are not associated with a viral infection but are common symptoms of beriberi (vitamin B1 deficiency).
- A leading authority says modern medicine’s denial that there are present-day dietary deficiency diseases in societies where there is food security has led to the plague called COVID-19. It is “high calorie malnutrition” that is killing Americans, not a coronavirus.
- The question of whether the COVID-19 coronavirus actually exists is questioned by other investigators.
- If the symptoms now being panned as COVID-19 really emanate from a dietary deficiency, all vaccines will predictably fail.
Since the inception of the COVID-19 lockdown measures, human populations have been suffering with an anxiety-induced syndrome that has increased an already prevalent B-vitamin deficiency, a nutrient that controls the autonomic nervous system that unconsciously controls heartbeat, breathing, digestion, and all the senses of smell, taste, touch and hearing.
The fear-evoking idea that a mutated cold-virus against which humanity had no immunity towards could swiftly induce breathlessness and take someone’s life away is something human populations of the world certainly can’t get off their minds. With no proven treatments or vaccines, the world is gripped with fear. The Grim Reaper delivers death even among seemingly healthy individuals. Who will be next?
But erase the COVID-19 case and death scoreboard and the fear that accompanies it. It’s all a ruse, a mass deception. Yes, people are dying, but not from a mutated coronavirus, or any coronavirus for that matter. The “co-morbidities” that accompany COVID-19, diabetes, heart disease, blood coagulation, kidney failure, are more likely the result of a change in dietary practices during lockdown than any imagined coronavirus.
We’re killing ourselves by eating and drinking ourselves to death
The lockdowns were predicted to generate 29-times more deaths than from the coronavirus itself.
Why?
What is causing many adults to die of breathlessness in hospital ICUs?
Results from a recent survey conducted by OnePoll market research, on behalf of a canned drinking water brand that adds hops and other “adaptogens” as a healthy alternative to beer, reveals COVID-19 is a lifestyle disease that brings on an anxiety-induced dietary and beverage changes.
The polling organization doesn’t realize all these changes in dietary practices block an essential nutrient needed for nervous system control.
The OnePoll survey reveals Americans are drinking more alcohol at home, consuming more “comfort foods” and swallowing down more coffee and tea to deal with fatigue and sleep loss.
The survey reveals 46% of those Americans working at home pour themselves an alcoholic drink during the workday; 53% of Americans are drinking more frequently during the lockdown.
Of particular interest is a survey which shows 52% of respondents felt a need to drink while watching the news on TV.
According to the National Institute on Alcohol Abuse & Alcoholism, there are 14.1 million American adults who have “alcohol use disorder.” Vitamin B1 deficiency is common among alcohol imbibers.
Two-in-five say also say they have been snacking more, and consuming “comfort foods.” That translates to “carbohydrates,” bread/pastry, rice, pasta, cereal.
Add 32% who claim they are drinking too much caffeinated beverages – – coffee and tea.
All of these anxiety/fatigue related foods and beverages interfere with vitamin B1 nutriture.
What started in Wuhan, China is not the COVID-19 of today
The COVID-19 coronavirus that started this worldwide pandemic in late 2019 is not the COVID-19 syndrome the public faces today during the lockdown era of the disease.
Bear with me a moment as I digress back to the start of the COVID-19 coronavirus outbreak. COVID-19 may have initially been panned as emanating from a mutated virus in Wuhan, China, where health authorities had been battling an outbreak of tuberculosis two years prior to COVID-19.
TB is, like COVID-19, a seasonal infectious lung disease, not caused by a virus but rather a mycobacterium.
TB could easily have been re-categorized as a COVID-19 coronavirus infection. Modena, Italy and New York City, two other COVID-19 geographic hotspots, were also plagued by prior TB outbreaks.
The Bacillus Calmette Guerin TB vaccine protects against COVID-19 infection, which also suggests TB cases were simply re-categorized as COVID-19. Oddly, nobody has raised suspicion that COVID-19 may simply be TB.
And what happened to Wuhan? There are barely any new cases in that city of 11 million people, while the US reports all-time high death counts.
Then came the lockdowns and what appeared to be a second round of COVID-19 that was in fact caused by the lockdowns themselves.
Loss of nervous system control
Vitamin B1 controls the autonomic nervous system – – heartbeat, breathing, digestion and elimination, and all the senses (touch/pain, smell, taste, hearing, vision). The chronic symptoms that characterize “long-haul” COVID – – headaches, crushing fatigue, loss of memory, weak muscles, are not associated with a viral infection but are common symptoms of beriberi (vitamin B1 deficiency).
✴︎
✴︎
Beriberi (vitamin B1 deficiency) is known as the great masquerader – it fools the best physicians. Over 120 years ago a vitamin B1 deficiency fooled doctors it was a viral disease because this dietary deficiency can cause the hypothalamus in the brain to produce a fever along with vomiting and diarrhea, symptoms commonly associated with viral infections.
The unconscious control of heart rate and breathing is lost. In this form of respiratory failure, the patient becomes breathless and simply dies as they can no longer stay awake and willfully control their breathing. Death is not caused by a so-called “cytokine storm” in the lungs of COVID-19-infected patients. It’s a nervous system problem, not an infection.
Why is zinc helpful if this is a vitamin B1 deficiency?
This author has widely touted zinc (particularly zinc lozenges) for COVID-19 prevention and treatment. But if COVID-19 symptoms are really being caused by a vitamin B1 (thiamine) deficiency and not an infectious viral disease, then why is zinc having a positive effect on the course of this vitamin-deficiency disease?
First, severe infections are common among thiamine-B1 deficient patients. These infections may be misleading pseudo-infections as manifestations of B1 deficiency, not true infections.
Remarkably, we find that zinc enhances the uptake of thiamine (vitamin B1) within cells.
Acute flaccid paralysis
There was another idiopathic (unexplained) paralytic nerve disease being reported throughout the US prior to the COVID-19 outbreak. It is called Acute Flaccid Paralysis (AFP), characterized by rapid onset of weakness of lower motor nerve cells (legs), with accompanying weakness of the respiratory and pharyngeal (swallowing) muscles, progressing to maximum severity within several days to weeks.
Acute flaccid myelitis (AFM) is believed to be caused by an infection with a type of virus known as an enterovirus. Respiratory illnesses and fever from enteroviruses are common — especially in children. Most people recover. It’s not clear why some people with an enterovirus infection develop acute flaccid myelitis.
From 2015 through 2017, 43 states reported 305 clinical cases. The CDC confirmed 193 pediatric AFM cases from 41 states, with most cases (143, 74%) reported in 2016
Overall, 161 (83%) patients had fever, cough, rhinorrhea (runny nose), vomiting, and/or diarrhea for a median of 5 days (range: 0 to 28 days) before limb weakness onset; 120 (62%) had fever, 127 (66%) had respiratory illness, and 45 (29%) had gastrointestinal illness.
In total, 106 patients (55%) had only 1 or 2 limbs affected compared with 87 patients (45%) who had 3 or 4 limbs affected 152 (79%) patients had at least 1 upper limb affected.
At the time of limb weakness onset, 63 (33%) patients also presented with cranial nerve findings, 69 (36%) had quadriplegia, 51(28%) had altered mental status, and 59 (33%) required mechanical ventilation. Twenty-eight (15%) had underlying medical conditions, of which 15 (8%) reported asthma. Only 1 of 81 patients who underwent a cerebral spinal fluid test was found to have a positive viral infection.
Acute flaccid paralysis is categorized as beriberi in Asia
Researchers in Asia call attention to patients who have similar symptoms ranging from weight loss, recurrent vomiting, profound weakness, anorexia, vocal cord dysfunction, side-to-side eye movements, mental confusion, who had a history of alcohol misuse that were successfully treated with thiamine vitamin B1.
Other researchers report severe flaccid paralysis is linked to thiamine deficiency. Modern medicine, steeped in its high technology, cannot diagnose a simple dietary deficiency disease like beriberi. In the US, this disease remains mysterious.
High calorie malnutrition
Derrick Lonsdale MD, the leading authority on vitamin B1, calls this syndrome “high calorie malnutrition” that strikes modern societies where there is an abundance of processed food, alcohol and sugar, but lacking essential nutrients.
At age 96 Dr. Lonsdale is still writing about thiamine, including its role in the COVID-19 pandemic.
When this author contacted Dr. Lonsdale to inquire whether COVID-19 isn’t really beriberi, he responded: “I couldn’t agree more.” Dr. Lonsdale is the author of the medical text: THIAMINE DEFICIENCY DISEASE, DYSAUTONOMIA, AND HIGH CALORIE MALNUTRITION.
Dr. Lonsdale wrote: “The medical profession is deaf to the idea because they are convinced that vitamin deficiency does not exist in America. How do you first cure widespread doctor deafness?” He says, for hospitalized and severe cases, mega-dose thiamine-B1 may be required. The real pandemic is “doctor denial.”
Vitamin B1 was discovered to be the cause of beriberi decades ago. Non-frontline doctors, with blinders on, are themselves dying because of failure to recognize the symptoms of beriberi. Modern medicine is making too much money off of beriberi to ever cure it or eradicate it, let alone recognize it walking in the office every day.
Does the COVID-19 coronavirus even exist?
Electron microscope images of the COVID-19 coronavirus have been brought into question.
While graphic images of the COVID-19 coronavirus show outward facing spikes, electron microscope images show these spikes face inwards in living cells. It is easy to misinterpret other intracellular structures as coronavirus particles. The news media has largely used fake images of COVID-19 coronavirus.
Neither does the current Polymerase Chain Reaction-PCR test reliably detect COVID-19. So, does COVID-19 really exist?
A thorough analysis of the test to detect COVID-19 coronavirus infection was conducted by Jesus Garcia Blanca (Discovery Health, November 2020). The original version of this report is in Spanish language but is reproduced in English at GreenMedInfo.
Dr. Blanca’s study reveals the genetic sequences (DNA letters) used in the polymerase chain reaction (PCR) test are present in the human genome itself and therefore the PCR test is worthless. The original sequence of COVID-19 virus corresponds to 74 sequences in the human genome, so it is not a novel mutation.
To date, a purified virus has not been produced to serve as a standard. The PCR test only detects fragments of human RNA, not COVID-19 in its entirety. None of the seven known coronaviruses have been isolated and characterized either.
All of the RNA sequences for COVID-19 have been found in other bacteria. One effort to isolate a coronavirus admits researchers “manually assembled and edited to produce a final sequence of the viral genome.” Therefore, no coronavirus can be held responsible for any disease. Maybe this is why no vaccine against any coronavirus has been licensed in the past decade.
Numerous inquiries into confirmation of the COVID-19 coronavirus at university databases have resulted in the same answer: “No record of work describing the isolation of the virus that is supposed to cause COVID19 can be found.”
Unequivocally a vitamin deficiency
Despite the clear evidence that the COVID-19 pandemic is a misdirection and the antidote is vitamin B1, this plague is aided and abetted by deniers of nutritional medicine. A 2014 landmark report in Scientific American questioned the “Health Impact of Vitamin Pill Remains Uncertain In A Developed World.”
It is unequivocal that the many symptoms of COVID-19 infection, which are system-wide (heart, kidneys, liver, brain, limbs), are not characteristic of a cold-virus but rather emanate from a dietary deficiency that was mistaken for a virus many decades ago when researchers attempted to explain the cause of beriberi.
If the COVID-19 deception is posited to be true, all vaccines will predictably fail. With a news media complicit in this ruse, will the world ever find out this pandemic is contrived? The cure is prevention with a 10-cent vitamin pill. Pro-vaccine billionaires who parade themselves as philanthropists be damned.
Instruction
Vitamin B1 is a water-soluble nutrient (thiamine hydrochloride) that is rapidly excreted. Diuretics (water pills, coffee) increase its excretion. Antacids for cases of heartburn impair B1 absorption. The anti-diabetic drug metformin also interferes with vitamin B1. Hence, we see a lot of diabetics among the patients who are hospitalized with COVID-19.
The superior forms of B1 dietary supplements are fat-soluble BENFOTIAMINE and ALLITHIAMINE, the latter passes through the blood-brain barrier. Essentially, all regular consumers of alcohol should be supplementing their diet with B1.
With the knowledge that Americans are consuming more processed foods and beverages that interfere with B1 nutriture, the Food & Nutrition Board is remiss in not increasing B1 food fortification.
More than 40 years ago the fortification of alcoholic beverages with thiamine B1 was proposed. More recently a leading medical ethicist has written a white paper entitled: The Case For Vitamin-Enriched Alcohol (Real Clear Science). This leads to my conclusion that Americans are being gamed for disease to treat. Preventive medicine is not practiced.
The dietary supplement industry is inexplicably as clueless to this beriberi epidemic as both alternative and conventional medicine, worsening the problem.
It is difficult to find fat-soluble forms of vitamin B1 on store shelves. It’s best to take B1 supplements at a different time than alcohol, coffee, tea, sugar, or medicines.
Beriberi is very circuitous. A shortage of thiamine-B1shuts down the sense of smell and taste and there is no hunger. The less food consumed the less B1. The lack of B1 shuts down secretion of stomach acid and less B1 is absorbed.
The unconscious control of heart rate and breathing is lost. In this form of respiratory failure, the patient becomes breathless and simply dies as they can no longer stay awake and willfully control their breathing. Death is not caused by a so-called “cytokine storm” in the lungs of COVID-19-infected patients. It’s a nervous system problem, not an infection.
Why is zinc helpful if this is a vitamin B1 deficiency?
This author has widely touted zinc (particularly zinc lozenges) for COVID-19 prevention and treatment. But if COVID-19 symptoms are really being caused by a vitamin B1 (thiamine) deficiency and not an infectious viral disease, then why is zinc having a positive effect on the course of this vitamin-deficiency disease?
First, severe infections are common among thiamine-B1 deficient patients. These infections may be misleading pseudo-infections as manifestations of B1 deficiency, not true infections.
Remarkably, we find that zinc enhances the uptake of thiamine (vitamin B1) within cells.
Acute flaccid paralysis
There was another idiopathic (unexplained) paralytic nerve disease being reported throughout the US prior to the COVID-19 outbreak. It is called Acute Flaccid Paralysis (AFP), characterized by rapid onset of weakness of lower motor nerve cells (legs), with accompanying weakness of the respiratory and pharyngeal (swallowing) muscles, progressing to maximum severity within several days to weeks.
Acute flaccid myelitis (AFM) is believed to be caused by an infection with a type of virus known as an enterovirus. Respiratory illnesses and fever from enteroviruses are common — especially in children. Most people recover. It’s not clear why some people with an enterovirus infection develop acute flaccid myelitis.
From 2015 through 2017, 43 states reported 305 clinical cases. The CDC confirmed 193 pediatric AFM cases from 41 states, with most cases (143, 74%) reported in 2016
Overall, 161 (83%) patients had fever, cough, rhinorrhea (runny nose), vomiting, and/or diarrhea for a median of 5 days (range: 0 to 28 days) before limb weakness onset; 120 (62%) had fever, 127 (66%) had respiratory illness, and 45 (29%) had gastrointestinal illness.
In total, 106 patients (55%) had only 1 or 2 limbs affected compared with 87 patients (45%) who had 3 or 4 limbs affected 152 (79%) patients had at least 1 upper limb affected.
At the time of limb weakness onset, 63 (33%) patients also presented with cranial nerve findings, 69 (36%) had quadriplegia, 51(28%) had altered mental status, and 59 (33%) required mechanical ventilation. Twenty-eight (15%) had underlying medical conditions, of which 15 (8%) reported asthma. Only 1 of 81 patients who underwent a cerebral spinal fluid test was found to have a positive viral infection.
Acute flaccid paralysis is categorized as beriberi in Asia
Researchers in Asia call attention to patients who have similar symptoms ranging from weight loss, recurrent vomiting, profound weakness, anorexia, vocal cord dysfunction, side-to-side eye movements, mental confusion, who had a history of alcohol misuse that were successfully treated with thiamine vitamin B1.
Other researchers report severe flaccid paralysis is linked to thiamine deficiency. Modern medicine, steeped in its high technology, cannot diagnose a simple dietary deficiency disease like beriberi. In the US, this disease remains mysterious.
High calorie malnutrition
Derrick Lonsdale MD, the leading authority on vitamin B1, calls this syndrome “high calorie malnutrition” that strikes modern societies where there is an abundance of processed food, alcohol and sugar, but lacking essential nutrients.
At age 96 Dr. Lonsdale is still writing about thiamine, including its role in the COVID-19 pandemic.
When this author contacted Dr. Lonsdale to inquire whether COVID-19 isn’t really beriberi, he responded: “I couldn’t agree more.” Dr. Lonsdale is the author of the medical text: THIAMINE DEFICIENCY DISEASE, DYSAUTONOMIA, AND HIGH CALORIE MALNUTRITION.
Dr. Lonsdale wrote: “The medical profession is deaf to the idea because they are convinced that vitamin deficiency does not exist in America. How do you first cure widespread doctor deafness?” He says, for hospitalized and severe cases, mega-dose thiamine-B1 may be required. The real pandemic is “doctor denial.”
Vitamin B1 was discovered to be the cause of beriberi decades ago. Non-frontline doctors, with blinders on, are themselves dying because of failure to recognize the symptoms of beriberi. Modern medicine is making too much money off of beriberi to ever cure it or eradicate it, let alone recognize it walking in the office every day.
Does the COVID-19 coronavirus even exist?
Electron microscope images of the COVID-19 coronavirus have been brought into question.
While graphic images of the COVID-19 coronavirus show outward facing spikes, electron microscope images show these spikes face inwards in living cells. It is easy to misinterpret other intracellular structures as coronavirus particles. The news media has largely used fake images of COVID-19 coronavirus.
Neither does the current Polymerase Chain Reaction-PCR test reliably detect COVID-19. So, does COVID-19 really exist?
A thorough analysis of the test to detect COVID-19 coronavirus infection was conducted by Jesus Garcia Blanca (Discovery Health, November 2020). The original version of this report is in Spanish language but is reproduced in English at GreenMedInfo.
Dr. Blanca’s study reveals the genetic sequences (DNA letters) used in the polymerase chain reaction (PCR) test are present in the human genome itself and therefore the PCR test is worthless. The original sequence of COVID-19 virus corresponds to 74 sequences in the human genome, so it is not a novel mutation.
To date, a purified virus has not been produced to serve as a standard. The PCR test only detects fragments of human RNA, not COVID-19 in its entirety. None of the seven known coronaviruses have been isolated and characterized either.
All of the RNA sequences for COVID-19 have been found in other bacteria. One effort to isolate a coronavirus admits researchers “manually assembled and edited to produce a final sequence of the viral genome.” Therefore, no coronavirus can be held responsible for any disease. Maybe this is why no vaccine against any coronavirus has been licensed in the past decade.
Numerous inquiries into confirmation of the COVID-19 coronavirus at university databases have resulted in the same answer: “No record of work describing the isolation of the virus that is supposed to cause COVID19 can be found.”
Unequivocally a vitamin deficiency
Despite the clear evidence that the COVID-19 pandemic is a misdirection and the antidote is vitamin B1, this plague is aided and abetted by deniers of nutritional medicine. A 2014 landmark report in Scientific American questioned the “Health Impact of Vitamin Pill Remains Uncertain In A Developed World.”
It is unequivocal that the many symptoms of COVID-19 infection, which are system-wide (heart, kidneys, liver, brain, limbs), are not characteristic of a cold-virus but rather emanate from a dietary deficiency that was mistaken for a virus many decades ago when researchers attempted to explain the cause of beriberi.
If the COVID-19 deception is posited to be true, all vaccines will predictably fail. With a news media complicit in this ruse, will the world ever find out this pandemic is contrived? The cure is prevention with a 10-cent vitamin pill. Pro-vaccine billionaires who parade themselves as philanthropists be damned.
Instruction
Vitamin B1 is a water-soluble nutrient (thiamine hydrochloride) that is rapidly excreted. Diuretics (water pills, coffee) increase its excretion. Antacids for cases of heartburn impair B1 absorption. The anti-diabetic drug metformin also interferes with vitamin B1. Hence, we see a lot of diabetics among the patients who are hospitalized with COVID-19.
The superior forms of B1 dietary supplements are fat-soluble BENFOTIAMINE and ALLITHIAMINE, the latter passes through the blood-brain barrier. Essentially, all regular consumers of alcohol should be supplementing their diet with B1.
With the knowledge that Americans are consuming more processed foods and beverages that interfere with B1 nutriture, the Food & Nutrition Board is remiss in not increasing B1 food fortification.
More than 40 years ago the fortification of alcoholic beverages with thiamine B1 was proposed. More recently a leading medical ethicist has written a white paper entitled: The Case For Vitamin-Enriched Alcohol (Real Clear Science). This leads to my conclusion that Americans are being gamed for disease to treat. Preventive medicine is not practiced.
The dietary supplement industry is inexplicably as clueless to this beriberi epidemic as both alternative and conventional medicine, worsening the problem.
It is difficult to find fat-soluble forms of vitamin B1 on store shelves. It’s best to take B1 supplements at a different time than alcohol, coffee, tea, sugar, or medicines.
Beriberi is very circuitous. A shortage of thiamine-B1shuts down the sense of smell and taste and there is no hunger. The less food consumed the less B1. The lack of B1 shuts down secretion of stomach acid and less B1 is absorbed.
✴︎
| COVID-19 coronavirus ... |
| Electron Microscopy.pdf |
✴︎
✴︎
✴︎
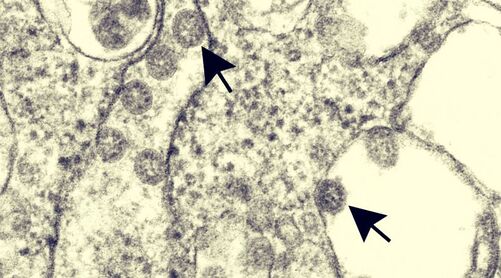
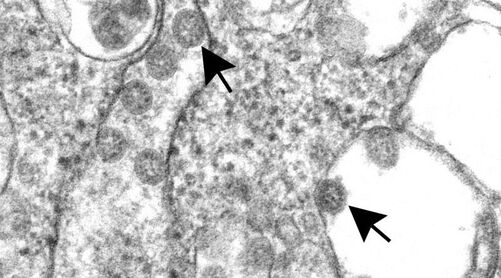
Figure: Viral isolate grown in cell culture Spherical coronavirus particles
with cross-sections through the nucleocapsid,
seen as black dots, are clustered within a membrane
which separates them from the cytoplasm.
✴︎
Figure: Viral isolate grown in cell culture Spherical coronavirus particles
with cross-sections through the nucleocapsid,
seen as black dots, are clustered within a membrane
which separates them from the cytoplasm.
✴︎
Electron microscopy of SARS-CoV-2:
a challenging task.
It is easy to misinterpret other intracellular structures as coronavirus particles.
We read with interest the Correspondence by Zsuzsanna Varga and colleagues on the possible infection of endothelial cells by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) using electron microscopic (EM) images as evidence.
However, we believe the EM images in the Correspondence do not show coronavirus particles but instead show cross-sections of the rough endoplasmic reticulum (RER).
These spherical structures are surrounded by dark dots, which might have been interpreted as spikes on coronavirus particles but are instead ribosomes.
The purported particles are free within the cytoplasm, whereas within a coronavirus-infected cell, accumulations of virus particles would be found in membrane-bound areas in the cisternae of the RER– Golgi area, where the spikes would be located on the inside of the cisternal space.
In addition, cross-sections through the viral nucleocapsid are not seen in the interior of these structures as would be found with coronavirus particles (figure). Just recently, there have been two additional reports 3,4 in which structures that can normally be found in the cytoplasm of a cell have been misinterpreted as viral particles.
EM can be a powerful tool to show evidence of infection by a virus, but care must be taken when interpreting cytoplasmic structures to correctly identify virus particles. We declare no competing interests.
The findings and conclusions are those of the authors and do not necessarily represent the position of the US Centers for Disease Control and Prevention.
It is easy to misinterpret other intracellular structures as coronavirus news media has largely used fake images of COVID-19 coronavirusparticles.
a challenging task.
It is easy to misinterpret other intracellular structures as coronavirus particles.
We read with interest the Correspondence by Zsuzsanna Varga and colleagues on the possible infection of endothelial cells by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) using electron microscopic (EM) images as evidence.
However, we believe the EM images in the Correspondence do not show coronavirus particles but instead show cross-sections of the rough endoplasmic reticulum (RER).
These spherical structures are surrounded by dark dots, which might have been interpreted as spikes on coronavirus particles but are instead ribosomes.
The purported particles are free within the cytoplasm, whereas within a coronavirus-infected cell, accumulations of virus particles would be found in membrane-bound areas in the cisternae of the RER– Golgi area, where the spikes would be located on the inside of the cisternal space.
In addition, cross-sections through the viral nucleocapsid are not seen in the interior of these structures as would be found with coronavirus particles (figure). Just recently, there have been two additional reports 3,4 in which structures that can normally be found in the cytoplasm of a cell have been misinterpreted as viral particles.
EM can be a powerful tool to show evidence of infection by a virus, but care must be taken when interpreting cytoplasmic structures to correctly identify virus particles. We declare no competing interests.
The findings and conclusions are those of the authors and do not necessarily represent the position of the US Centers for Disease Control and Prevention.
It is easy to misinterpret other intracellular structures as coronavirus news media has largely used fake images of COVID-19 coronavirusparticles.
✴︎
✴︎